Tavsif
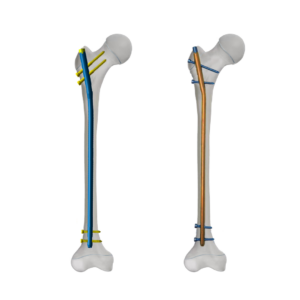
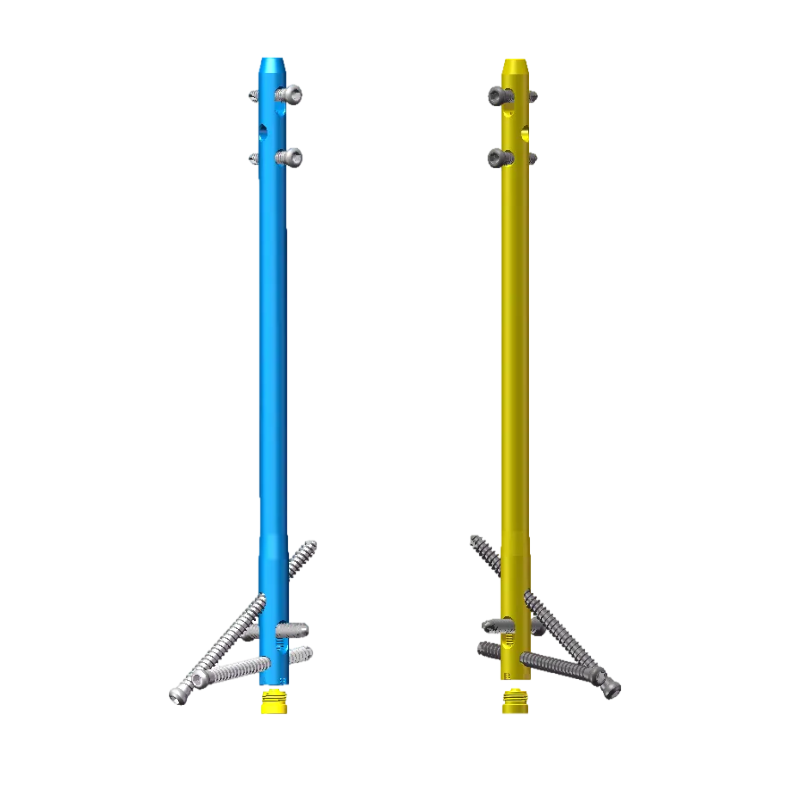
To'piq artrodez mix
Sh&A
1-chora: What is the primary indication for using an Ankle Arthrodesis Nail?
A1: It is most common in patients with severe, end-stage hindfoot arthritis, Charcot neuroarthropathy, major post-traumatic deformity, or as a salvage following failed previous surgeries.
2-savol: What is the definitive anatomical goal of Tibiotalocalcaneal
arthrodesis?
A2: The goal is to achieve a solid, well-aligned bony fusion between the tibia, talus, and calcaneus using a nail inserted retrograde from the calcaneus into the tibial medullary canal.
So'ymoq: What is the typical surgical approach and entry point for tibiotalocalcaneal (TTC) retrograd nail?
A3: The standard approach is a posterior or plantar heel pad incision, with the entry point typically at the calcaneal tuberosity, aiming precisely to align the mechanical axis and avoid neurovascular structures.
Q4: How critical is preoperative planning, and what specific assessments are needed?
A4: It is absolutely critical. Preop must include assessment of bone quality, limb alignment, vascular status, and precise templating to choose nail length/diameter and screw trajectories, often using CT scans.
Q5: What is the postoperative weight-bearing protocol, and how long until fusion is expected?
A5: Patients are typically kept non-weight-bearing for 6-12 weeks, progressing to full weight-bearing by 3-4 months once radiographic fusion is confirmed, which usually takes 4-6 oylar.
Chora: What are the alternatives to an ankle fusion nail, and when are they preferred?
A6: Alternatives include external fixation (for severe infection) and screw/plate constructs (for isolated tibiotalar fusion without subtalar involvement). Plates may be preferred when the subtalar joint is to be preserved.
Q7: What is the role of bone graft in hindfoot nailing?
A7: Autograft or allograft is essential to fill any bone defects, promote biologics, and increase the surface area for fusion, especially in atrophic nonunions or after resection of necrotic bone.