Introduction
Pediatric diaphyseal femur fractures are among the most common long bone injuries in children and adolescents. З сучаснымі артапедычнымі імплантатамі, two main fixation systems are used: the Elastic Stable Intramedullary Nailing (РЭЛІГІЯ) and the Падлеткавы бакавы ўваход у сцегнавы пазногаць (АЛФН). Understanding their indications and biomechanical differences is essential for achieving optimal healing and functional recovery.
1. Definition and AO Classification
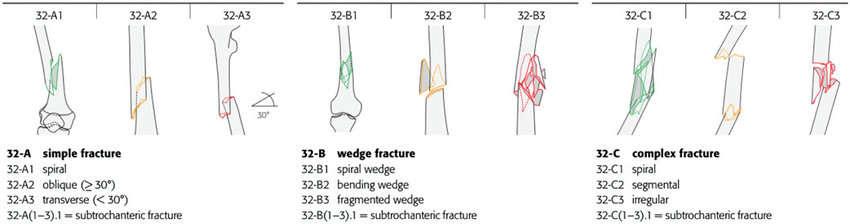
Diaphyseal femur fractures occur in the shaft (mid-diaphysis) of the femur and are classified by the AO/OTA system as group 32 with subgroups A (simple), Б (wedge) і С (multifragmentary), a useful framework for operative planning and prognosis.
2. Pediatric Interlocking Intramedullary Nail (АЛФН)
The Падлеткавы бакавы ўваход у сцегнавы пазногаць (АЛФН) is a pediatric interlocking intramedullary nail designed for adolescents nearing skeletal maturity.
Перавагі:
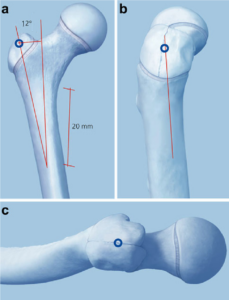
Lateral entry point minimizes risk to the femoral head blood supply.
Interlocking options ensure excellent axial and rotational control.
Rigid fixation allows for early mobilization and faster rehabilitation.
Паказанні:
Length-unstable diaphyseal femur fractures
Comminuted fractures
Heavier or older children (>45 kg)
The adolescent femoral nail provides superior stability when flexible fixation is insufficient.
3. Elastic Stable Intramedullary Nailing (РЭЛІГІЯ)
The Elastic Stable Intramedullary Nail (РЭЛІГІЯ), commonly known as the elastic nail, remains the gold standard for pediatric femur fractures in younger children.
Перавагі:
Minimally invasive with smaller incisions and shorter operation time.
Elastic fixation promotes micro-motion, enhancing callus formation.
Preservation of bone biology, as no reaming is required.
Паказанні:
Length-stable diaphyseal fractures
Children aged 5–11 years
Patients with moderate body weight and high remodeling potential
4. Choosing Between ALFN and ESIN
Choose ESIN when the patient is younger, lighter, and the fracture is length-stable (AO 32-A, transverse/short oblique). Перавагі: minimally invasive, low morbidity, fast recovery.
Disadvantages: may fail to control length/rotation in heavy adolescents or in comminuted fractures.
Choose pediatric interlocking intramedullary nail with lateral entry(АЛФН ) when the patient is an adolescent (or heavier child >45–50 kg), the fracture is length-unstable or comminuted (AO 32-B/C), or when early full weight-bearing and robust rotational control are desired.
Перавагі: superior axial and rotational stability, lateral entry reduces AVN risk, earlier ambulation;
Disadvantages: greater implant cost, need for interlocking technique and fluoroscopic control, and careful consideration in skeletally immature proximal femoral physes.
5. Выснова
Comparative case series and reviews show ESIN yields excellent outcomes in the appropriate younger population, while lateral-entry rigid adolescent nails produce reliable union and shorter time to full weight-bearing in older/heavier children with low observed AVN rates in published series. Clinical decision should therefore be individualized by age, weight, fracture pattern (AO class), and surgeon expertise.
Note:The copyright belongs to the original author and the magazine,posts are for learning and communication only.