1. Introduction
The LCP Paediatric Hip Plate (PFP) features a universal design suitable for both left and right femurs, making it highly versatile for paediatric orthopaedic procedures. It is available in three system, tailored to the patient’s age and body weight:
2.7 mm plate: For infants and toddlers weighing up to 15 kg
3.5 mm plate: For children aged 3–8 years, typically up to 35 kg
5.0 mm plate: For older children and adolescents
The system offers multiple angular options to address a range of deformities and indications:
Varus correction: 100° or 110°
Valgus correction: 130°,140°,150°
Rotational osteotomies & femoral neck fractures: 120°
2.Conditions Treated with the Paediatric Hip Plate
The paediatric proximal femur is affected by various congenital and acquired pathologies, which often require surgical intervention. These include:
Developmental Dysplasia of the Hip (DDH): A congenital condition where the hip socket is shallow or malformed.
Neuropathic Hip Dysplasia: Common in cerebral palsy, leading to instability and deformity.
Slipped Capital Femoral Epiphysis (SCFE): A disorder of the growth plate causing displacement of the femoral head.
Perthes’ Disease: Avascular necrosis of the femoral head in children.
Femoral Neck Fractures: Often due to high-energy trauma.
Post-tumor resection deformity and congenital pseudarthrosis.
Early surgical correction of these conditions is crucial to ensure normal gait, prevent pain, and preserve joint function.
3.Indications and Contraindications
Indications:
Intertrochanteric or subtrochanteric varus/valgus osteotomies
Rotational osteotomies for femoral anteversion or retroversion
Open reduction and internal fixation of displaced femoral neck fractures
Deformity correction after SCFE or tumor resection
Patients requiring angular and rotational stability
Contraindications:
Active infection at the surgical site
Severely compromised bone quality (e.g., severe osteogenesis imperfecta)
Skeletal immaturity without appropriate indication
Allergy to titanium (rare)
4.Case Overview
Case 1:
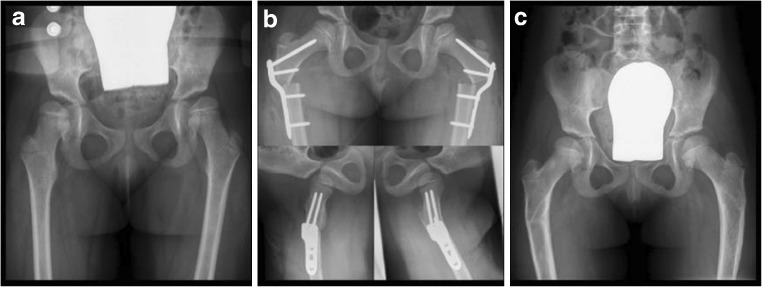
A 4-year-old girl with cerebral palsy. a Bilateral subluxation due to valgus deformity of the femoral shaft. b A bilateral intertrochanteric varus osteotomy together with a derotation was performed. c The postoperative course was uneventful, and the plates could be removed bilaterally 5 months after the initial operation
Case 2:
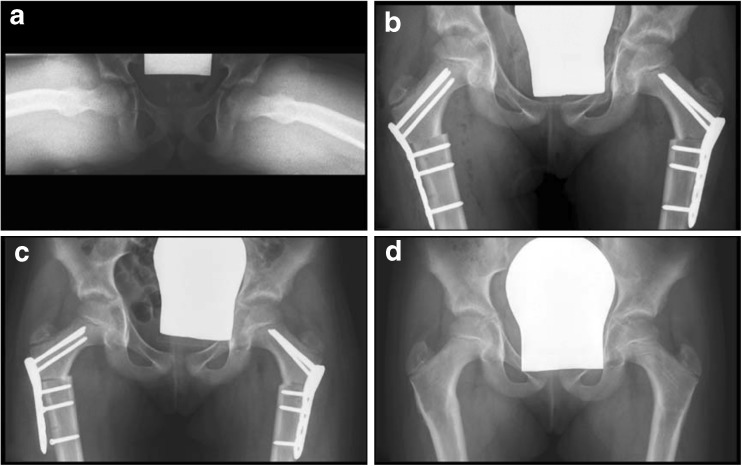
a A 9.5-year-old girl with bilateral idiopathic retroversion of 10°. b A bilateral derotation osteotomy was done and fixed by a 3.5-mm 120° LCP Paediatric Hip Plate. c Two weeks after the operation, the girl complained of right-sided pain in the proximal femur. The X-ray showed loosening of the femoral shaft screws from the DC holes. d A revision was performed to change and refix the plate. The further course was uneventful with plate removal 10 months after the initial operation
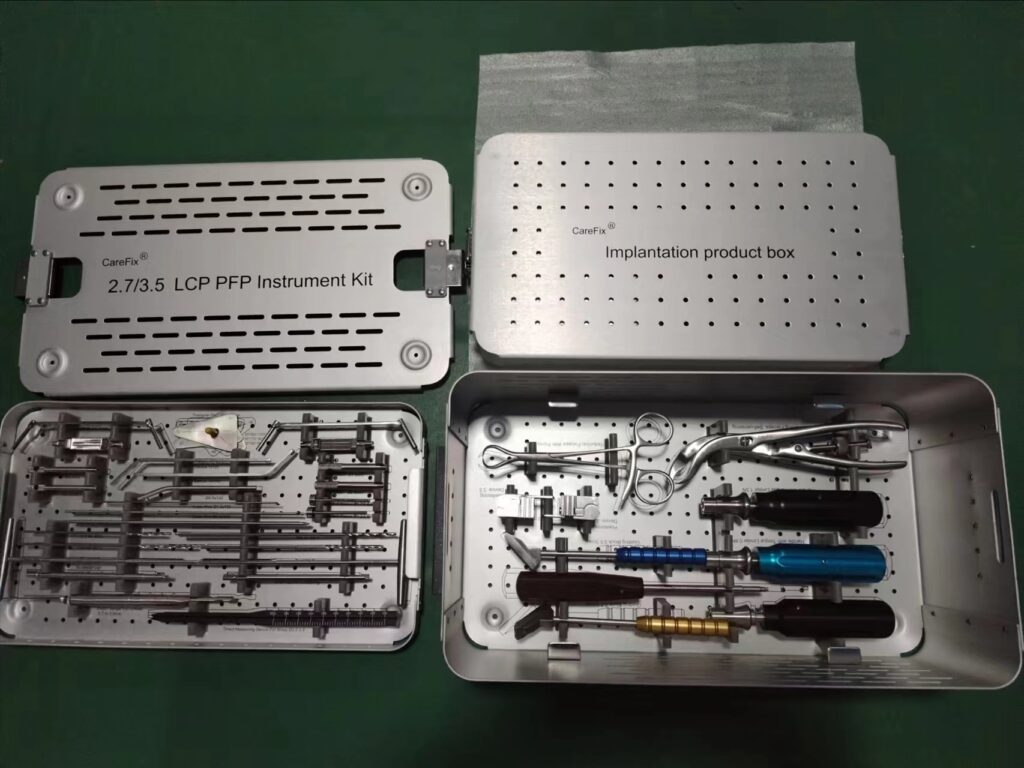
5.LCP Proksimal Femoral Plaka (PFP)Tool Kit
6. Conclusion
The LCP Paediatric Hip Plate™ (Paediatric PFP) has proven to be a safe, versatile, and effective titanium locking plate for managing deformities and fractures of the paediatric proximal femur. Compared to traditional systems like angular blade plate or external fixator, the plate offers:
Improved angular stability
Simplified surgical workflow
Excellent correction precision
Low complication rates
As more paediatric orthopaedic surgeons adopt this system, it is likely to become the standard of care for treating complex femoral deformities in children.