AO Type C3 Distal Radius Fractures
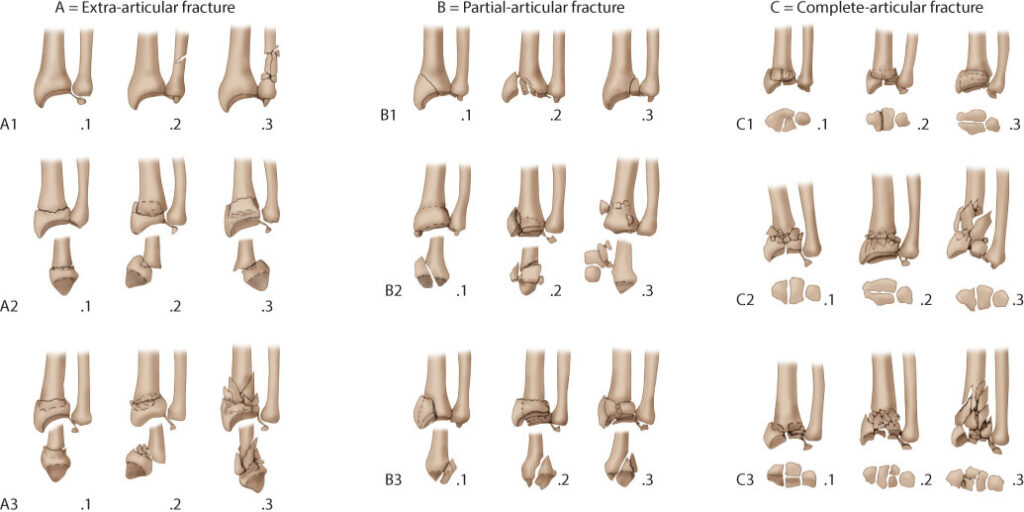
Distal radius fractures are among the most common orthopedic injuries worldwide, especially in older adults following low-energy trauma or in younger individuals due to high-impact injuries. According to the AOclassification, distal radius fractures are divided into types A (extra-articular), B (partial articular), và C (complete articular). AO type C3 is the most complex subtype, involving comminuted intra-articular fractures with a high risk of displacement, shortening, and joint incongruity.
Managing these fractures poses significant challenges, as they often require both strong anatomical fixation and support against axial loading and collapse. To address this, the combination of a Volar Locking Plate and a Distal Radius Fixator has shown promising outcomes in stabilizing such complex fractures while allowing early wrist mobilization.
Tấm bán kính xa LCP Volar
The LCP (Locking Compression Plate) Volar Distal Radius Plate is anatomically contoured to fit the volar aspect of the distal radius. It provides angular stability through locking screws, particularly important in osteoporotic bone and comminuted fractures. The plate acts as a stable buttress to prevent volar displacement and aids in maintaining articular congruity.
Bộ cố định bán kính xa
The Distal Radius Fixator is an external fixation device, often incorporating a double-ball joint mechanism, allowing postoperative controlled wrist movement. Originally introduced by Pennig in 1993, the dynamic transarticular fixator has evolved as a solution to maintain distraction and prevent radial collapse while permitting functional rehabilitation.
Thuận lợi
1.Combined mechanical stability from the internal VLP and external fixator
2.Early mobilization through dynamic wrist motion postoperatively
3.Maintains radial height and articular congruity, especially in comminuted fractures
4.Minimizes soft tissue disruption compared to fragment-specific plating
5.Effective in osteoporotic bone
chỉ định
1.AO Type C2/C3 distal radius fractures
2.Comminuted intra-articular fractures
3.Unstable fractures at risk of collapse
4.Patients requiring early range-of-motion rehabilitation
Chống chỉ định
1.Open fractures with severe contamination
2.Poor soft tissue conditions preventing safe external fixator pin placement
3.Uncooperative patients or those unable to comply with postoperative care
4.Pre-existing wrist infections
Clinical Outcomes
A study involving 11 patients (mean age: 61 years) treated with this combined method demonstrated encouraging results:
1.Wrist Extension/Flexion: Mean 76°/64°
2.Grip Strength: 84% compared to the contralateral side
3.Modified Mayo Wrist Score: Mean 88 (good to excellent function)
4.DASH Score: Mean 9 (minimal disability)
5.Radiographic Assessment: No significant loss of reduction or articular congruity at final follow-up
6.Fixator Removal Time: 3–6 weeks (mean 5 weeks)
7.Rehabilitation: Initiated on day one postoperatively, improving functional outcomes and reducing joint stiffness
The external fixator functioned as a static stabilizer for two weeks and then as a dynamic mobilizer, preserving length and articular congruency during early motion exercises.
Phần kết luận
The combination of the LCP Volar Distal Radius Plate and the Distal Radius Fixator provides a robust and adaptable treatment strategy for managing complex AO Type C3 distal radius fractures. While the VLP offers internal structural support and anatomic alignment, the external fixator maintains distraction forces and enables early wrist mobilization,essential in preventing joint stiffness and promoting functional recovery.
This dual approach bridges the gap between rigid fixation and functional rehabilitation, making it particularly valuable for difficult fracture patterns in both elderly and active adult population.