Midshaft Clavicular Fracture
Clavicle fractures are common fractures, which comprise 3% к 5% of all fractures, и 44% of fractures in the shoulder region in adults. In total, 65% к 80% of these fractures are located in the middle third, и 94% are caused by a direct blow to the shoulder.
Why Choose MIPO technology
The clavicle is a membranous bone with a predominantly periosteal vascular supply, and extensive periosteal stripping during open surgery may lead to nonunion and infection. Closed reduction and internal fixation can minimize the aforementioned complications. Intramedullary nailing is one option, but it doesn’t maintain well the length or rotation in comminuted fractures, and nail migration or breakage may lead to dangerous complications.
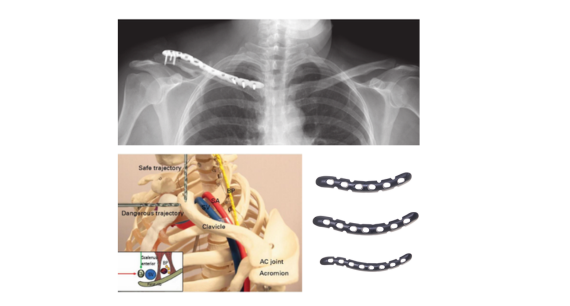
Because of the popularity of biological fracture fixation, which leads to better fracture healing, the minimally-invasive plate osteosynthesis (MIPO) technique is being applied to the management of clavicular shaft fractures.And according to the AO principle, it is necessary to restore the length of the clavicle, axial alignment and rotation of the clavicle, and bridge the clavicle with locking plate without complete anatomical reduction of the midshaft fracture of the multi-segment or crushed clavicle. This provides a theoretical basis for MIPO treatment of clavicular fracture.
Traditional open reduction and internal fixation surgery trauma is bigger, is easy to damage the supraclavicular nerves, with the development of the concept of minimally invasive and patient demand for local aesthetics, MIPO technology more widely applied in clavicle fractures.
Advantages
1.Surgical wound is small and incision is short.
2.Less disruptive to periosteum stripping, less blood supply.
3.Avoid supraclavicular nerve injury.
4.Provide excellent biological healing and optimal stabilisation strength.
Postoperative Care
1. Immobilization and Early Protection
Sling support: After surgery, the shoulder is usually protected with a sling for about 2 weeks. This reduces stress on the healing bone and decreases pain.
Early mobilization: Even during the immobilization phase, patients are encouraged to perform pendulum exercises, which gently move the shoulder joint and help maintain mobility.
2. Gradual Return to Activities
Daily activities: Light daily activities, such as using the hand for eating or writing, are typically allowed at 4 weeks postoperatively.
Restrictions: Lifting weights or carrying heavy objects with the injured arm is strictly forbidden until bone union is confirmed.
3. Follow-Up and Monitoring
Schedule: Patients are generally reviewed at 4, 8, и 12 weeks after surgery.
X-ray evaluation: Anteroposterior radiographs of the clavicle are taken to assess bone healing.
Union criteria: Bone healing is confirmed by both radiological evidence (bony bridging between fracture fragments) and clinical signs (absence of tenderness, improved shoulder function).
4. Healing Timeline
On average, fracture union occurs within 8–15 weeks (mean around 11 weeks).
Delayed union: Callus formation seen after 24 weeks.
Nonunion: No visible callus and abnormal mobility after 24 weeks.